As parents, we are often very concerned about many different aspects of our child’s life. We are stressed about their physical well being, their intellectual development, their social skill sets. In Singapore, one of the most pressing concern is the development and progression of myopia or more commonly known as short-sightness.
Myopia is the result of the elongation of the eyeball, causing distant objects to be blurry. Severe myopia increases the risk of developing future eye problems such as retinal detachment, glaucoma etc. The development and progression of myopia is multi-factorial. The current research has pointed to 3 main factors, of which 2 is modifiable
a) Genes – there are to date 24 myopic risk genetic factors. Individuals who have a higher myopia risk factor gene count has a 1000% increase in developing myopia
b) Lack of outdoor activities under the sun
c) Increase in near activities such as reading, digital devices, Lego bricks, drawing
The last 2 factors are modifiable risk factors. This means that parents can have the option to reduce the probability of myopia development and/or to slow the progression by increasing the outdoor activities and reducing the amount of near vision activities. Should these methods prove to be ineffective or insufficient, there are other modes of myopia control that is available.
1) Ophthalmic lenses
a) Zeiss Myovision
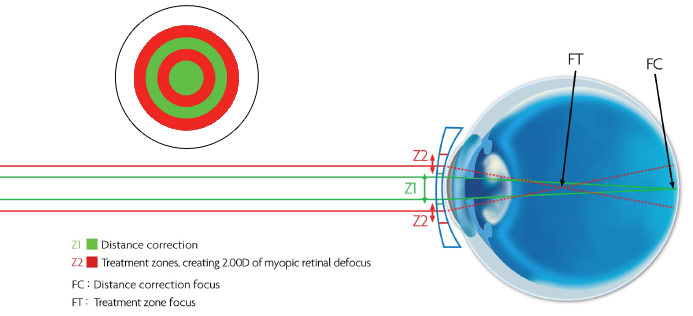
The theory suggests that in a myopic eye, correction with a traditional device such as a spectacle lens causes the image to focus on the retina centrally but comes to a focus behind the retina at the periphery resulting in blur that could drive the eye to elongate and for myopia to increase. The lens designs reversed this by moving the peripheral image forward, onto or in front of the retina, while simultaneously positioning the central image on the retina, resulting in clear vision. A 30% reduction in myopic progression in two hundred 6-12 year olds with a history of parental myopia was seen with one of the designs.
http://journals.lww.com/optvissci/Fulltext/2010/09000/Spectacle_Lenses_Designed_to_Reduce_Progression_of.4.aspx
For Myovision to work well, the centering of the glasses is of utmost importance. The fitting of the frame should be firm and not sliding the bridge to ensure that the center clear zone is at eye point. Little or no adaptation is required. At our practice, we would recommend this lenses if the myopia progression is not rapid.
b) Add lenses such as Progressives or bifocals
Progressives lenses work to reduce accommodation on a young child whilst reading. These lenses will work fairly well if the accommodative convergence ratio (aka AC/A ratio) is higher than normal. However, the main issue with progressive lenses is that it is difficult to ensure that the young child is using the correct lower prescription of these lenses to read. Bifocals will be a better choice than progressives as it allows the child to access the full reading zone easily. The frames selected should be well fitting to ensure that the child can access the reading zone easily. Progressive lenses may not be the ideal choice for children with exotropia (outward squint)
c) Prismatic Bifocals (Myopilux Max)
Prismatic Bifocals work to reduce accommodation as well as reduce accommodation and the need to convergence (which drives accommodation again). These lenses are easy to adapt but the visible line may become a cosmetic concern with kids as they grow older. These lenses ARE not suitable for young children with convergence excess (inward squint) problems.
2) Medical Means
Atropine used in varying dosage may retard progression of myopia in children. The most recent study of 0.01% atropine suggest that it is effective in slowing myopia progression with minimal side effects. We usually notice a very slight increase of about 1-2 mm increase pupil size especially so in lighter irises. Photo grey lenses may be then prescribed to alleviate the glare from ambient light.
During subsequent reviews, should the 0.01% not be as effective as desired, the ophthalmologist may suggest changing to a stronger atropine dosage such as 0.1%, 0.125% or even 1%. Most of the time, we do see better results in terms of stabilising/ slowing down the progression of myopia when this course of action is taken. However, these children will experience a larger pupillary dilation and a more relaxed/ sluggish accomodation. This results in them feeling more glare and a noticeable effort to switch focus between distance to near vision. They will likely need photogrey lenses with bifocal or progressive lenses to cope with the academic demands while on such treatment.
Atropine treatment is not be desirable for kids who exhibit a outward squint for either distance or near. Kids with history of eczema may need a closer monitoring to ensure that the eyedrops does not trigger any allergies around the eye.
3) Orthokeratology
Ortho-K lenses is a special gas permeable lenses that moulds the shape of the cornea to create a peripheral defocus. These lenses are typically worn to sleep to effect a change on the cornea. The lenses will be removed during waking hours and the patient will be able to have good vision throughout the day. In order for the effects to sustain, the patient has to be on such lenses every night. Ortho-k has been very effective at controlling the myopia progression if well fitted. Hence it is very important to choose the right orthokerathologist.
However, with overnight wear of lenses, there will be a small but recurring risk of eye infections. The orthokerathologist and child, with the assistance of the parents must work together to reduce the risk. The most pressing concern amongst practitioners and parents is the development of microbial keratitis. Hence, Ortho-K lenses should be treated as a medical device and there must be regular follow up with the optometrist.
4) Bates programme
Highly controversial…. most of the results has been anecdotal without any clinical trials or even studies done. Certain part of the programme that encourages good visual habits, rotation of the eyeball and exposure to sun may by useful to relax the eye muscles or secretion of dopamine that may have a similar effect to atropine.
So… are you more confused?
Bring your child to an optometrist for a consult and check what myopia control may be most suitable for your child. Do remember that clinical decisions and emotive decisions can differ and these influences the options.
updated 12th November 2017